Clinical Psychologist for Individuals, Couples, Families, Groups & Professionals
How Therapy Helped Reduce OCD Distress During a Major Life Change: An Anonymised Case Study
Can therapy help OCD? This is an anonymised clinical case study. Identifying details have been changed. It is not a promise of similar results. Therapy outcomes vary depending on severity, history, motivation, treatment fit, and life context.
In my work, I sometimes meet people whose OCD is not only distressing in the mind, but deeply disruptive in daily life. The person may look outwardly functional, yet inwardly be trapped in relentless doubt, guilt, checking, and fear. This anonymised case reflects that kind of suffering.
The patient was a woman in her mid-30s who came to therapy with severe obsessive-compulsive symptoms, especially harm-related obsessions. She was repeatedly troubled by intrusive fears that she may have harmed someone unknowingly or unintentionally. These thoughts were not wishes or intentions. They were ego-dystonic, frightening, and experienced as alien to her values. Yet because they produced intense guilt and doubt, she felt driven to check, review, and seek certainty.
Her OCD also affected ordinary functioning. Leaving the house could become difficult. Everyday movement was interrupted by intrusive fears about danger, contamination, hazard, or having failed to notice something unsafe. The result was not only anxiety, but mental exhaustion, low mood, and a shrinking of life around fear.
“When OCD becomes organized around guilt and responsibility, the person is not only afraid of danger. They are afraid of being the cause of danger.” — Tejas Shah
What the scores suggested initially
At the start of therapy, her questionnaire profile suggested substantial distress across OCD, mood, anxiety, and related symptom domains.
Two other points are worth noting because honest case writing should not flatten complexity. Somatization rose slightly from 3 to 5, and hostility rose from 5 to 6, remaining elevated. That does not cancel the overall improvement, but it reminds us that change in therapy is rarely a perfectly neat downward line across every domain.
Clinically, the initial profile suggested a person carrying:
severe OCD distress, especially around harm, responsibility, and checking
marked guilt and anxiety
depressive symptoms likely related to chronic mental strain, reduced freedom, and repeated internal alarm
sensitivity to life transitions and heightened fear under uncertainty
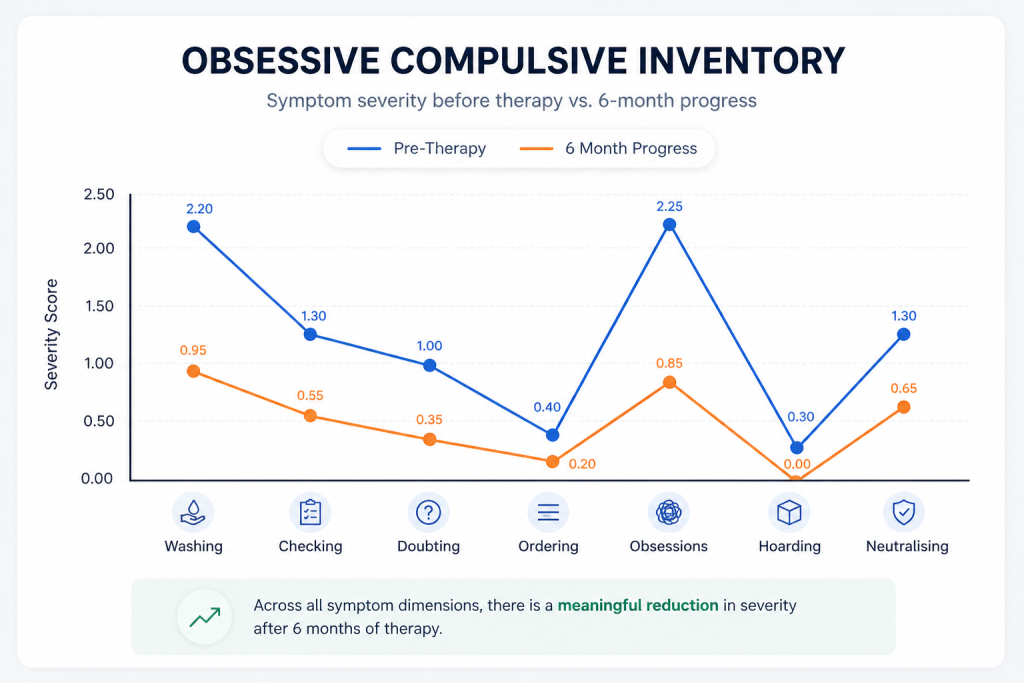
The OCI subscale pattern suggested that before therapy, the patient was especially burdened by intrusive obsessions, washing-related distress, checking, and neutralising rituals. After therapy, all major OCD domains showed reduction, with the largest changes seen in obsessional distress and compulsive responding. This suggests not simply less anxiety in a broad sense, but a meaningful reduction in the specific OCD cycle that had been shaping her daily life.
The pattern underneath the symptoms
One useful way to understand OCD is to look not only at the symptom, but at what keeps recreating it.
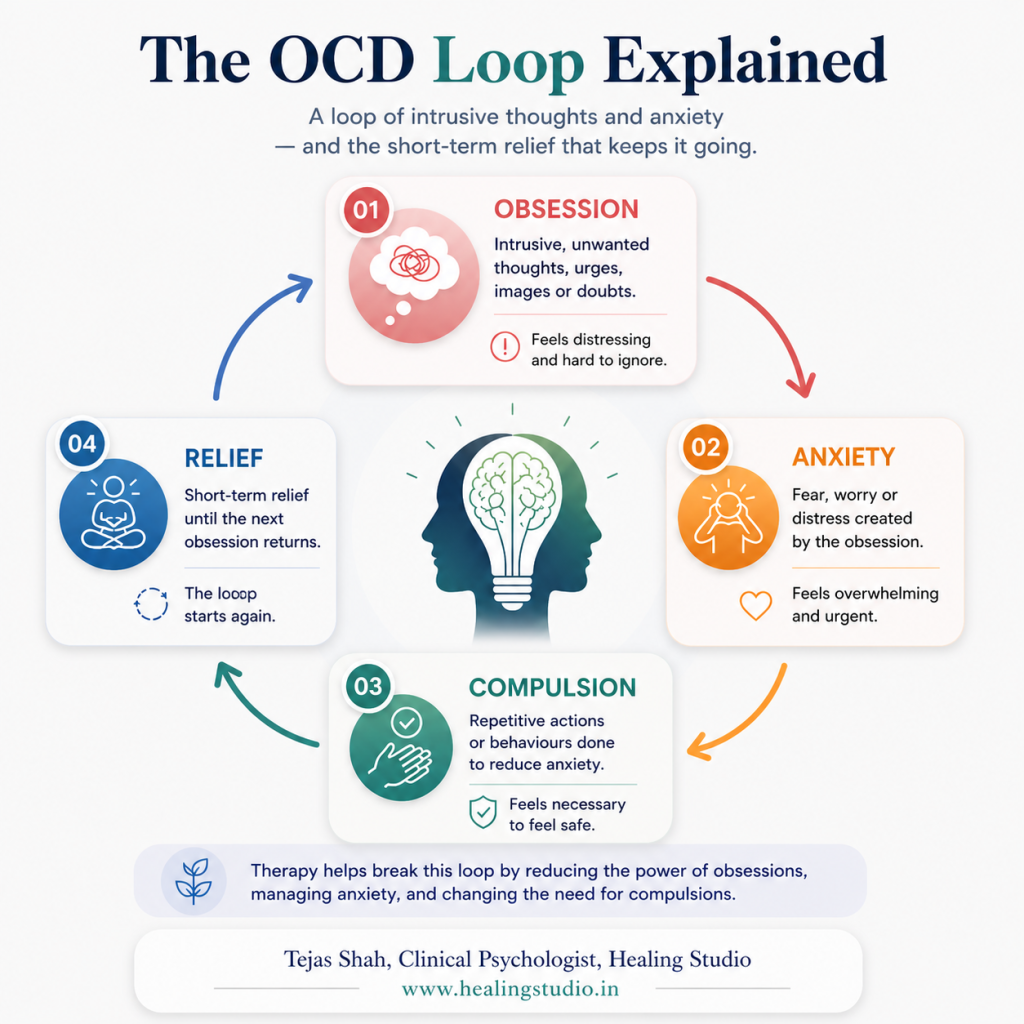
The OCD Loop
In this case, the visible symptom was harm-related obsessional thinking and checking. The maintaining pattern underneath it was a loop: an intrusive thought appeared, guilt surged, doubt expanded, checking followed, temporary relief came, and then the mind learned to treat the original fear as important and unfinished. The next thought then arrived with even more force.
That is why reassurance alone rarely solves the problem for long. It reduces anxiety briefly, but often feeds the cycle by teaching the mind that certainty must be achieved before one can feel safe.
Can therapy help OCD? How I approached the therapy
I worked integratively, drawing from both psychodynamic and cognitive approaches.
The cognitive side of the work involved helping her understand intrusive thoughts more accurately, recognize the guilt-checking cycle, and gradually relate differently to the urge for certainty. We worked on the difference between a thought and an action, between doubt and evidence, and between responsibility and impossible moral perfection.
The psychodynamic side of the work mattered too. In some forms of OCD, especially harm OCD, there is often more going on than fear alone. There may also be conflict around aggression, conscience, guilt, control, and the need to be absolutely safe or morally beyond reproach. Therapy helped make space for these deeper emotional meanings without treating the patient as dangerous or defective. That distinction is crucial.
In clinical work, this is rarely just a problem of “irrational thinking.” It is often a problem of fear, guilt, responsibility, and emotional regulation becoming fused into a punishing inner system. Can therapy help OCD? Integrative therapy can help by addressing both the thought process and the emotional structure that keeps giving the thought its force.
“Effective OCD work is not about proving safety perfectly. It is about changing the relationship to doubt, guilt, and urgency.” — Tejas Shah
What changed after therapy
The clearest changes were in OCD burden, anxiety, depressive symptoms, and real-life functioning.
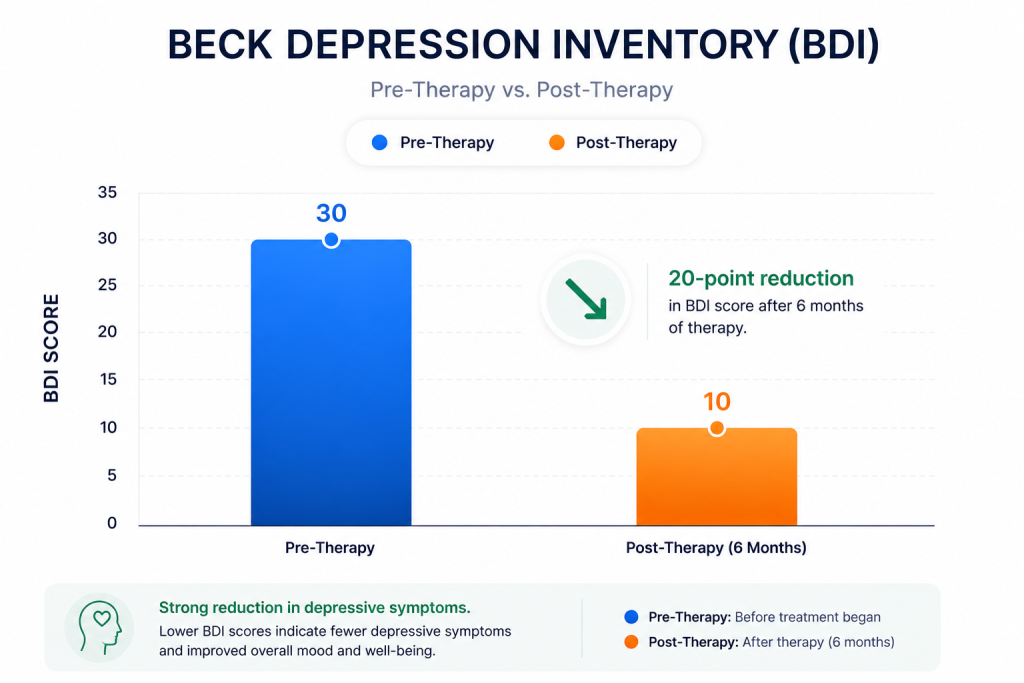
The OCI score reduced from 62 to 26. In simple terms, this suggests that obsessive-compulsive symptoms became substantially less consuming. The BDI reduced from 30 to 10, suggesting that the emotional heaviness surrounding the OCD also improved significantly.
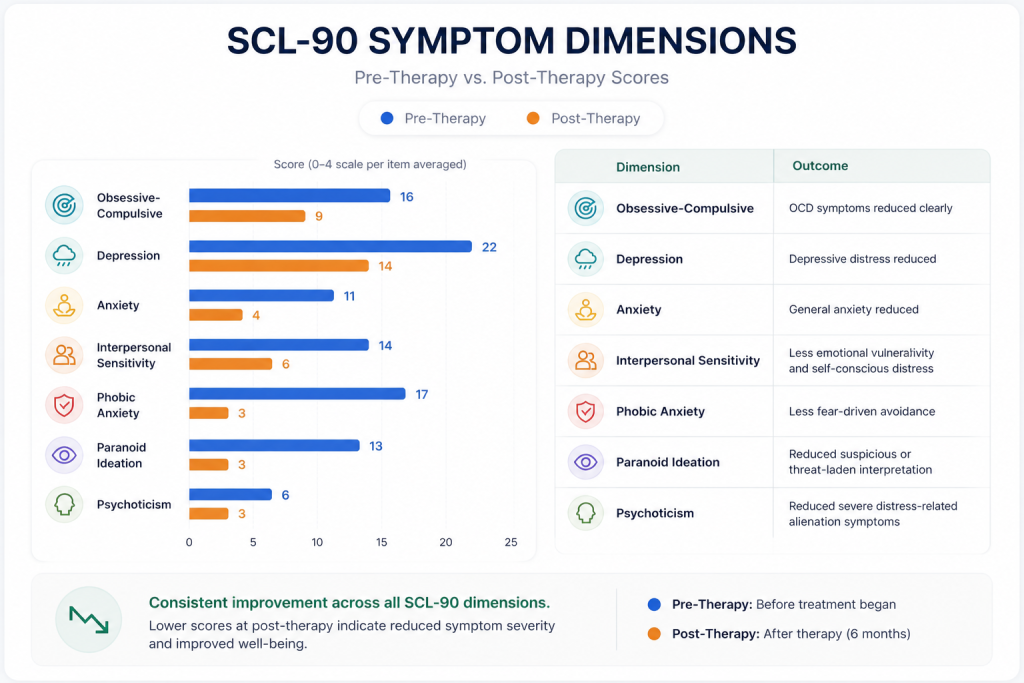
The SCL-90 pattern broadly moved in the same direction. Obsessive-compulsive symptoms reduced. Anxiety reduced. Depression reduced. Interpersonal sensitivity reduced. Fear-driven avoidance reduced sharply. Threat-based or suspicious interpretations reduced. Overall, the post-therapy profile suggested a mind that was less flooded, less trapped, and less controlled by repetitive fear.
What matters most, however, is not only that the scores moved. It is that the patient’s way of meeting life began to change.
The SCL-90 profile suggests broad post-therapy improvement across the main areas of distress. The most marked reductions were seen in phobic anxiety, indicating substantially less fear-driven avoidance, and in paranoid ideation, suggesting reduced threat-based or suspicious interpretation under stress. There were also clear reductions in obsessive-compulsive symptoms, general anxiety, and depressive distress, consistent with a less burdened and less internally preoccupied psychological state. Improvement in interpersonal sensitivity suggests reduced emotional vulnerability, shame-proneness, and self-conscious distress in relation to others. The reduction in psychoticism is best understood here not as evidence of a psychotic disorder, but as a decrease in severe distress-related alienation, inner disorganization, or unusual subjective discomfort. Overall, the pattern is consistent with meaningful symptomatic improvement, better emotional regulation, and reduced psychological strain across both core OCD symptoms and associated distress domains.
Can therapy help OCD? A real-life outcome moment
After a major relocation, she reached out with a follow-up message. She described that this kind of life event would earlier have intensified her OCD significantly. This time, however, she reported that the symptoms were minimal and that she was able to go through the move with a much calmer mind. She also expressed deep gratitude for the treatment.
Patient’s WhatsApp Message (anonymized, summarized and recreated)
That follow-up mattered clinically because relocation is not a trivial test. Major transitions often activate OCD strongly: uncertainty rises, routines change, vigilance increases, and the mind becomes more vulnerable to catastrophic doubt. The fact that she could move through such an event with far less takeover by OCD suggests something important.
This is what improvement can look like in real life: not the absence of all anxiety, but the capacity to move through a stressful life event without OCD taking over. – Tejas Shah
That kind of outcome is often more meaningful than symptom scores alone. A questionnaire may tell us that distress reduced. Real-life functioning tells us whether the person can actually live differently when life becomes demanding again.
What this may mean clinically
This case suggests meaningful therapeutic improvement, not a miracle and not a guaranteed template.
Clinically, the change may indicate:
reduced fusion with intrusive harm thoughts
reduced compulsive checking and fear-based responding
improved emotional regulation under stress
less guilt-driven escalation
improved functioning during a major life transition
less depressive collapse secondary to chronic OCD distress
It may also suggest that therapy helped not only at the level of symptom management, but at the level of inner organization. The patient appears to have become less governed by urgency, fear, and compulsive responsibility, and more able to remain psychologically steady under pressure.
The BDI score reduced from 30 to 10, suggesting a substantial reduction in depressive symptom burden after therapy. Clinically, the pre-therapy score was consistent with significant depressive distress, likely reflecting emotional heaviness, exhaustion, hopelessness, guilt, and the secondary impact of chronic OCD-related strain on mood and functioning. The post-therapy score suggests that depressive symptoms became much less severe, with improvement in overall mood, mental burden, and day-to-day coping. This does not imply that all sadness, stress, or vulnerability disappeared. Rather, it suggests that the patient was less weighed down by depressive suffering and had regained a greater degree of emotional steadiness, functioning, and psychological room to manage life.
What cannot be concluded from one case
Can therapy help OCD? One case can be clinically meaningful, but it has limits.
This report does not show that therapy “cures” OCD. It does not prove that every person with harm OCD will improve in the same way. It does not tell us which single element of therapy produced the change, or whether the same gains will remain stable under every future stress. It also does not mean that all symptoms disappeared.
In addition, some symptom domains did not move in a simple direction. That matters. Therapy outcomes are often uneven. A person may improve markedly in one area while still carrying strain in another.
Why this case matters
I am careful with case studies. The value of a case like this is modest and, in my view, more useful.
It shows how OCD can present as guilt, fear, checking, avoidance, and shrinking freedom. It shows how depression can build around obsessive suffering. It shows why therapy may need to address both symptom loops and deeper emotional dynamics. And it shows that improvement is often best judged not by perfection, but by whether a person can live with more steadiness, more freedom, and less domination by fear.
Can Therapy Help OCD? What Improvement Can Look Like
In this anonymised case, I worked with a woman in her mid-30s who was struggling with severe OCD, especially harm-related intrusive thoughts, guilt, checking, and difficulty leaving the house without fear-driven distress. Her pre-therapy scores suggested a high burden of obsessive-compulsive and depressive symptoms (OCI 62, BDI 30). After integrative therapy using psychodynamic and cognitive approaches, her post-therapy scores showed substantial reduction in OCD and mood distress (OCI 26, BDI 10), with broader improvement across anxiety-related symptom domains. So, can therapy help OCD? Most importantly, during a major relocation that would previously have worsened her OCD, she reported being able to go through the transition with a much calmer mind and minimal symptom escalation. This is what meaningful improvement can look like in practice: not perfection, but greater freedom, steadiness, and functioning under real-life stress.
FAQs
1. Does this OCD case study mean therapy can cure OCD?
No. This case does not imply cure. It shows meaningful improvement in one anonymised case, including reduced OCI and BDI scores and better functioning during a stressful life transition. OCD outcomes vary depending on severity, history, treatment fit, consistency, medication, life stress, and other clinical factors.
2. What is harm OCD?
Harm OCD involves unwanted intrusive thoughts or fears about harming someone, causing danger, or being responsible for harm. These thoughts are usually deeply distressing and inconsistent with the person’s values. The person may then check, avoid, review, or seek reassurance to reduce guilt and uncertainty.
3. Why did depressive symptoms reduce along with OCD symptoms?
In some cases, depression worsens when OCD becomes exhausting, restrictive, and guilt-filled. When obsessive-compulsive distress reduces, mood may also improve because the person feels less trapped, less ashamed, and more able to function. However, depression may also need direct clinical attention in its own right.
4. Why is real-life functioning important in OCD recovery?
Scores are useful, but they are not the whole story. OCD recovery also needs to be seen in daily life: leaving the house, tolerating uncertainty, reducing checking, handling transitions, and continuing with life even when anxiety appears. Functioning shows whether change is entering real situations, not only questionnaires.
When OCD Starts Taking Over Daily Life
If intrusive thoughts, checking, guilt, or fear of harm are affecting your ability to live freely, individual therapy may help you understand the pattern and work with it more steadily. Therapy is not about proving that every fear is impossible. It is about changing how your mind responds to doubt, guilt, and uncertainty.
You may consider exploring Individual Therapy at Healing Studio if OCD, anxiety, overthinking, or depressive symptoms are interfering with your daily functioning.
This article is educational in nature and cannot replace therapy, diagnosis, or an individualized clinical assessment. The case is anonymised, shared with written consent, and presented to illustrate one pattern of therapeutic improvement rather than to promise a similar outcome for others.
Tejas Shah is an RCI-Licensed Clinical Psychologist, Therapist, Founder and Clinical Director of Healing Studio, with over 16,000 hours of therapeutic experience. He works with individuals struggling with OCD, intrusive thoughts, anxiety, depression, guilt, emotional regulation, and deeper personality or relational patterns. His work integrates psychodynamic understanding with cognitive and practical therapeutic approaches, helping clients move toward greater clarity, steadiness, and real-life functioning.
Explore Therapy at Healing Studio
If this article reflects something important in your life, therapy may offer a space to understand it more clearly and work with it in depth.
Individual Therapy Support for anxiety, depression, trauma, emotional struggles, self-criticism, and deeply rooted personal difficulties.
Couples Therapy Support for conflict, resentment, disconnection, trust difficulties, and repetitive relationship patterns.
Found this article helpful? Follow My WhatsApp Channel for brief reflections on mental health, relationships, emotions, and updates on new articles/workshops:
Related Posts:
How Therapy Can Help with Exam Anxiety and Performance Pressure Exam anxiety is not just “stress.” For many students, it becomes a cycle of pressure, overthinking, poor sleep, self-doubt, and difficulty functioning. This article explains what may be keeping that cycle alive and how therapy can help.
Undermined at Work: What Happens When Someone Quietly… Not all workplace sabotage is loud or easy to prove. Sometimes it looks like delay, non-cooperation, quiet exclusion, procedural obstruction, or being made to look unreliable. This article explores what being undermined at work does to the mind, why it becomes so hard to switch off, and how therapy may help.
How to Deal With a Coworker Who Keeps Blocking Your Work When a coworker keeps delaying, resisting, withholding, or quietly obstructing progress, the stress is not just practical. It can create helplessness, rage, self-doubt, and obsessive overthinking. This article explains why that dynamic becomes so consuming—and how to respond more clearly.
When an Online Gaming Friendship Starts Feeling… An online gaming friendship can become deeply meaningful. This article explores why that bond may start to feel unusually powerful, why online friends matter so much, and when emotional closeness begins turning into emotional dependency.
Published by
Tejas Shah
TEJAS SHAH is a PhD Scholar and has M.Phil in Clinical Psychology (RCI), MSc in Psychology, MA in Philosophy and a Degree in Law (LL.B) from University of Mumbai; he is practicing as Chief Clinical Psychologist at Healing Studio. His research interests are consciousness, phenomenology, positive psychology, philosophical counselling and mindfulness. You can connect with him on [email protected].
View all posts by Tejas Shah